Menu
Menu

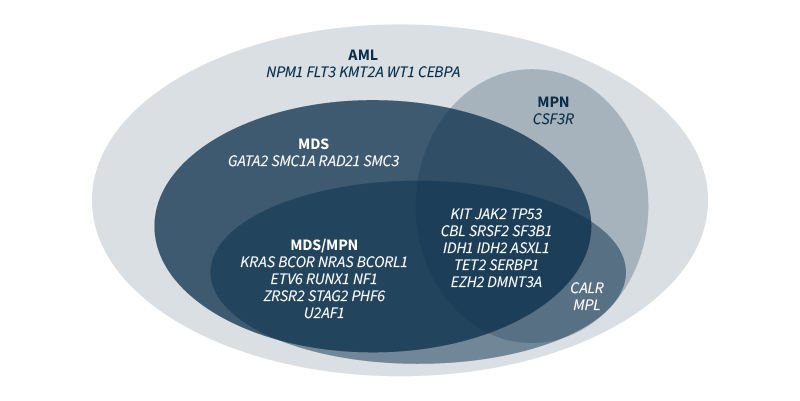
Myeloid malignancies or neoplasms are rare clonal disorders of hematopoietic stem or progenitor cells. They are caused by genetic and epigenetic changes that disrupt fundamental cellular processes, such as self-renewal, differentiation, and proliferation.1 Mutations encountered in myeloid malignancies include somatic variants, such as single nucleotide variants (SNVs), insertions and deletions (Indels), gene fusions, and copy number variations (CNVs). Some of the genetic changes are strongly associated with a specific phenotype (e.g., BCR/ABL fusion in chronic myeloid leukemia), but most are not linked to a single diagnostic entity (Figure 1).2
Accurate detection of mutations is extremely important for the diagnosis and prognosis of myeloid malignancies, and to identify the genomic events that are classified as ‘actionable’, i.e., those for which targeted therapies exist. The advent of next generation sequencing (NGS)-based techniques greatly enhanced our capability to detect mutations. There are numerous advantages of using NGS: it is a high-throughput method that allows for massive parallel sequencing of multiple targeted genomic regions in many samples, shortening the time to report. Moreover, differently to traditional methods, an NGS analysis requires small amounts of tumor DNA/RNA. However, NGS has also brought about some challenges.
Mutations and their patterns in myeloid malignancies are heterogeneous and must be identified, warranting the use of NGS for their detection. Ensuring that a gene panel is comprehensive enough to detect all variants implicated in myeloid neoplasms is one of the biggest challenges for a clinical laboratory performing molecular testing of new or suspected cases.2 Compiling a gene list is a tall order that requires a careful analysis of recent publications, FDA-approved targeted therapies, scientific society guidelines, and the products and services offered by NGS companies. A balance is needed – a very large gene panel will be expensive to run and time-consuming to analyze, whilst a small panel may miss important information.
SOPHiA GENETICS offers offers expertly designed applications with key genes associated with hematological malignancies, and also supports healthcare institutions in the design of custom applications with the desired gene content to fully meet their research needs.
Three genes are notoriously difficult to assess by NGS in myeloid neoplasm samples: FLT3, CEBPA, and CALR. Challenges with FLT3 internal tandem duplication (ITD) mutation detection derive from difficulties in aligning sequence reads with large duplications. Moreover, larger duplications are missed by amplicon-based panels, if the sequencing read is shorter than the ITD size. As FLT3-ITD length has a prognostic value, the identification of the ITD must be precise. False negatives in CEBPA mutation detection are often encountered in assays that are not carefully designed and validated, whereas CALR is problematic in NGS due to difficulties in detecting Indels resulting in frameshift mutations, e.g., a common 52bp deletion variant.2 Complex genes require optimal probe design, coverage and analytic pipelines.
Complex genes require optimal probe design, coverage and analytic pipelines.
The SOPHiA DDM™ for Blood Cancers portfolio has been designed to offer uniform coverage of complex genomic variants to ultimately allow:
A timely identification of mutations is of crucial importance for two genes in particular: TP53 and FLT3. A mutation in TP53 correlates with chemoresistance and identifies patients in whom standard therapy will do more harm than good. Timely identification of FLT3-ITD is needed to introduce a recently approved treatment with a specific kinase inhibitor that must be administered on day 8 of the induction therapy.2 However, the average laboratory turnaround time for NGS assays is 13 to 21 days, which makes NGS-based FLT3 detection unfeasible for first-line treatment decisions.2 To solve this challenge, continuous optimization of all aspects of the laboratory workflow is needed.
The advanced analytics of SOPHiA DDM™ provide optimized variant detection in a single workflow. For example, the SOPHiA DDM™ for Blood Cancer applications have been trained to efficiently detect all FLT3 fragment sizes, irrespective of the insertion point. All confirmed ITDs were detected (no false negatives) and no additional variant was called (no false positives), making it a robust and reliable detection method.
In addition to the technical challenges described above, a laboratory performing NGS-based mutation profiling in myeloid neoplasms faces several variant interpretation problems. NGS techniques result in a huge number of genetic variants needing interpretation, which requires a significant amount of time and expertise from institutions. Also, many genes may acquire novel mutations that are not present in NGS databases. Often, such mutations are classified as variants of uncertain significance and are of little value for the prognosis and guidance on therapeutic choices. Computational prediction algorithms can help institutions identify and understand biologically relevant, actionable biomarkers. All such analyses should be incorporated into the bioinformatic pipeline to produce the end report for the clinician.3
Computational prediction algorithms can help institutions identify and understand biologically relevant, actionable biomarkers
With the SOPHiA DDM™ Platform, experts can flag the pathogenicity level of variants. Flagging decisions are supported by access to SOPHiA GENETICS’ global community of knowledge sharing and qualified databases containing relevant information on the variants, including those of unknown significance.
SOPHiA GENETICS products are for Research Use Only and not for use in diagnostic procedures unless specified otherwise.
SOPHiA DDM™ Dx Hereditary Cancer Solution, SOPHiA DDM™ Dx RNAtarget Oncology Solution and SOPHiA DDM™ Dx Homologous Recombination Deficiency Solution are available as CE-IVD products for In Vitro Diagnostic Use in the European Economic Area (EEA), the United Kingdom and Switzerland. SOPHiA DDM™ Dx Myeloid Solution and SOPHiA DDM™ Dx Solid Tumor Solution are available as CE-IVD products for In Vitro Diagnostic Use in the EEA, the United Kingdom, Switzerland, and Israel. Information about products that may or may not be available in different countries and if applicable, may or may not have received approval or market clearance by a governmental regulatory body for different indications for use. Please contact us to obtain the appropriate product information for your country of residence.
All third-party trademarks listed by SOPHiA GENETICS remain the property of their respective owners. Unless specifically identified as such, SOPHiA GENETICS’ use of third-party trademarks does not indicate any relationship, sponsorship, or endorsement between SOPHiA GENETICS and the owners of these trademarks. Any references by SOPHiA GENETICS to third-party trademarks is to identify the corresponding third-party goods and/or services and shall be considered nominative fair use under the trademark law.